



Hardware components | ||||||
_wzec989qrF.jpg?auto=compress%2Cformat&w=48&h=48&fit=fill&bg=ffffff) |
| × | 1 | |||
| × | 1 | ||||
 |
| × | 1 | |||
 |
| × | 1 | |||
 |
| × | 1 | |||
Hand tools and fabrication machines | ||||||
 |
| |||||
 |
| |||||
 |
| |||||
I created a device using liquid lenses allowing for the glasses to change its prescription. Because of this ability, these glasses can determine an individual's prescription and change to correct vision for different prescriptions. This device eliminates the need for progressive/bifocal lenses and yearly eyeglass/contact replacements.
ABSTRACTA third of the world’s population has poor vision and can’t obtain visual aids, negatively impacting economies and societies. People also use multifocal eyeglasses instead of using multiple glasses with various prescriptions. Although multifocal lenses combat the need for multiple glasses, it confines vision by only providing users a narrow field to view objects. These glasses cause eye strain/fatigue and chronic neck problems/pain. This project aims to create a device that can integrate a voltage-controlled liquid lens to change lens curvature to mimic phoropters and multifocal visual aids without their associated problems. Data obtained on the “percent increase in visual acuity” in relation to participants' original visual acuity show that the average increase using auto focal glasses (58.06%) was significantly higher than the average increase using current visual aids (41.33%). This difference was determined to be significant showing with 95% confidence that the device was able to improve vision in comparison to commonly used visual aids. This device improves vision as it allows for finer adjustments to be made by the user to focus light on to the optic nerve. The device was also effective in improving vision due to the blocking of stray light caused by the reduced aperture of the lens which increases visual acuity. In conclusion, this auto focal visual aid improved a user’s vision significantly more than the user’s current visual aids as these auto focal glasses can adjust and adapt to the user’s current visual needs.
INTRODUCTIONA third of the world population has poor vision, and most people with poor vision are unable to obtain eyeglasses to correct their vision (Chen, p. 1). Poor vision has a serious impact on economies by reducing GDP and increasing the frequency of fatal accidents. One major problem that is faced by people is that they are unable to determine their eye prescription. This is because many local optometrists don't have access to expensive equipment, such as the phoropter, to determine an individual's prescription. People who use glasses require visual correction due to the inflexibility of their natural lens and/or weakened Ciliary muscles. When the natural lens becomes inflexible or the Ciliary muscles of an eye become weak, the eye is unable to bend the natural lens enough to focus all the incoming light rays onto the optic nerve. The focal point of light falls behind or in front of the optic nerve rather than directly on it. Most people wear glasses to solve this problem and help their eyes direct light onto the optic nerve. Under certain circumstances, users use progressive or multifocal glasses, which use lenses that have sections that transition between different lens prescriptions for viewing objects in various ranges (Figure 1.1). Although the usage of progressive and multifocal glasses can combat the need for multiple glasses, it greatly confines viewing experience by only allowing users to look through narrow bands to see certain objects in focus. These glasses also cause eye strain/fatigue and lead to chronic neck problems/pain (Zetterberg, Forsman, & Richter, 2017).Presbyopia is a common problem where the eye is unable to focus on nearby objects. It is caused by gradual thickening and loss of flexibility of the natural lens. This leads to the eye being unable to focus on nearby objects and still retain the ability to focus on distant objects. As they age, many presbyopic patients also lose their ability to focus on objects far away requiring them to obtain a special type of visual aid. To combat this common problem that occurs with old age, individuals rely on bifocal lenses. These were first invented as a revolutionary solution, allowing users to switch to one pair of eyeglasses for all their needs opposed to having different glasses for looking at different things. These glasses work by having certain portions of the glass have a different power, thus supporting different prescriptions based on the direction in which the user looks (Figure 1.1: Different Lens Structures).
Currently, progressive glasses are used in the same manner and provide a smoother transition allowing the user to focus on objects at a range of distances from the user. Although these types of glasses are useful, they also greatly limit vision by restricting the user to view through narrow bands to look at objects at particular distances causing eye fatigue and chronic neck pain. Phoropters are machines that have precisely machined lenses to aid in determining an individuals’ eye prescription (Figure 1.2: Image of Phoropter). This machine, invented 200 years ago, determines eye prescription by cycling through multiple sets of lenses to find a lens that will best correct the patient’s vision. Although the phoropter is widely used and is still able to provide accurate prescriptions, it is large and not a portable, ergonomic nor a cost-effective solution to provide prescriptions to those who need them.
Engineering Goal: To create a device that can effectively integrate a voltage-controlled variable focus lens and microcontroller to automatically change lens curvature with the use of a program. This device would replace phoropters and be used as an autofocus eyeglass that adjusts the focal length of a variable focus lens to allow for clarity of vision when looking at different ranges, replacing progressive and multifocal visual aids. It was hypothesized that the auto focal visual aid created would improve a user’s vision significantly in comparison to the user’s current visual aids as auto focal glasses can adjust and adapt to the user’s current visual needs. A lens is a transparent substance with curved sides that can concentrate or disperse light due to its refractive properties. A focal point is a point at which parallel light rays converge after passing through a lens and the focal length is the distance between the center of the lens and the focal point. Eye prescription is given in Powers which is measured in diopters. Power =1/Focal length. The human eye’s lens is attached to the Ciliary muscles (Reece, Urry, & Cain, 2018). These muscles around the lens contract and relax to change lens curvature. By changing the lens curvature, the ciliary muscles can focus incoming light onto the optic nerve. The thicker the center of the lens is relative to the edges of the lens, the more the lens refracts light and reduces the focal length and vice versa. As shown in Figure 1.3 when the seen object is closer to the eye, the Ciliary muscles contract to make the lens thicker to focus the diverging light rays on the Retina. Also shown in Figure 1.3, when the seen object is further from the eye, the Ciliary muscles relax to make the lens flat, focusing the nearly parallel light rays on the optic nerve. When the natural lens is unable to bend enough to focus light onto the optic nerve, glasses are needed. Placing glasses in front of eyes direct incoming light onto the optic nerve. This reduces the amount of strain and effort that the eye has to go through to direct incoming light.
A lens that uses fluids to create an infinitely-variable lens with no moving parts is known as a liquid lens. Liquid lenses use a process called electrowetting to change the curvature of the lens (Varioptic, n.d., p. 1). Wetting is the property of a liquid to maintain contact with a solid surface. The level of wetting is defined by a force balance between cohesive and adhesive forces. Electrowetting is the modification of wetting properties with the use of electric potential (voltage). By manipulating the wetting properties of water, a polar substance, the shape and the curvature of the liquid can change as the water hugs or repels the surfaces of the lens. The liquid lens contains two insoluble liquids: water and a non-conductive oil separated by a film. As shown in Figure 1.4, applying a voltage to the film between the liquids changes the curvature, and therefore the focal length. As more voltage is applied to the lens, the lens bends more increasing the optical power of the lens and vice versa.
In this device, the microcontroller will calculate the necessary voltage to send to the lens. Given the prescription of the user or digital input, the microcontroller will automatically adjust the voltage provided to the lens changing its focal length accordingly. This use of the device will replace the need for cumbersome multifocal and progressive lenses. To find the prescription of a user, the microcontroller will cycle through different voltages, gradually increasing voltage and decreasing the focal length (Figure 1.4). Once the focal point of light falls on the optic nerve, the user will be able to see with a high degree of visual acuity (sharpness of vision). Once the user can see at a high degree of visual acuity, the user would press a button on the IR remote indicating to the device to calculate the prescription of the user. This allows the device to know which voltage was best suited to correct for their vision and would be able to calculate the user's power knowing the amount of voltage provided to the lens and thus the curvature of the lens, focus, and power of the lens.
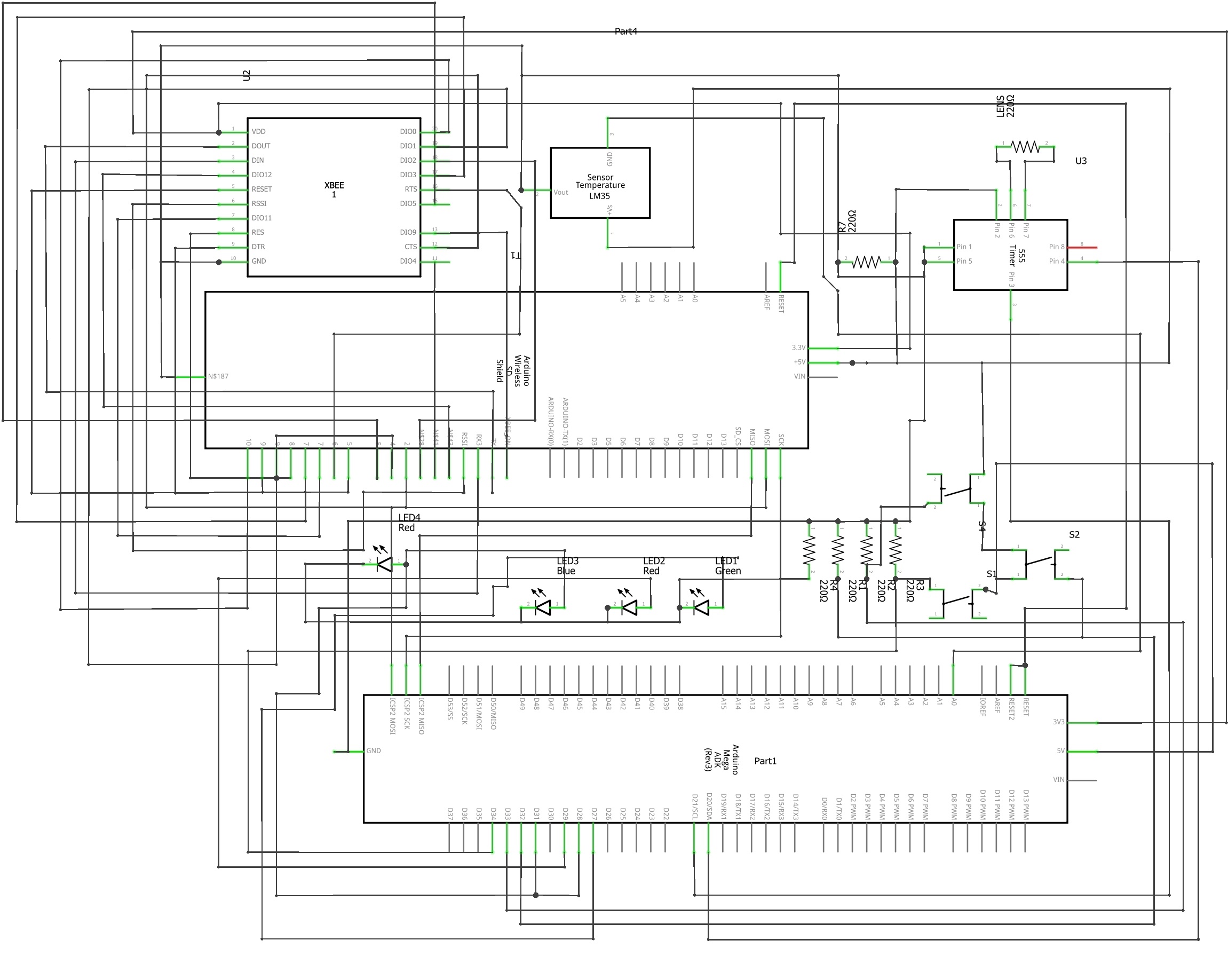
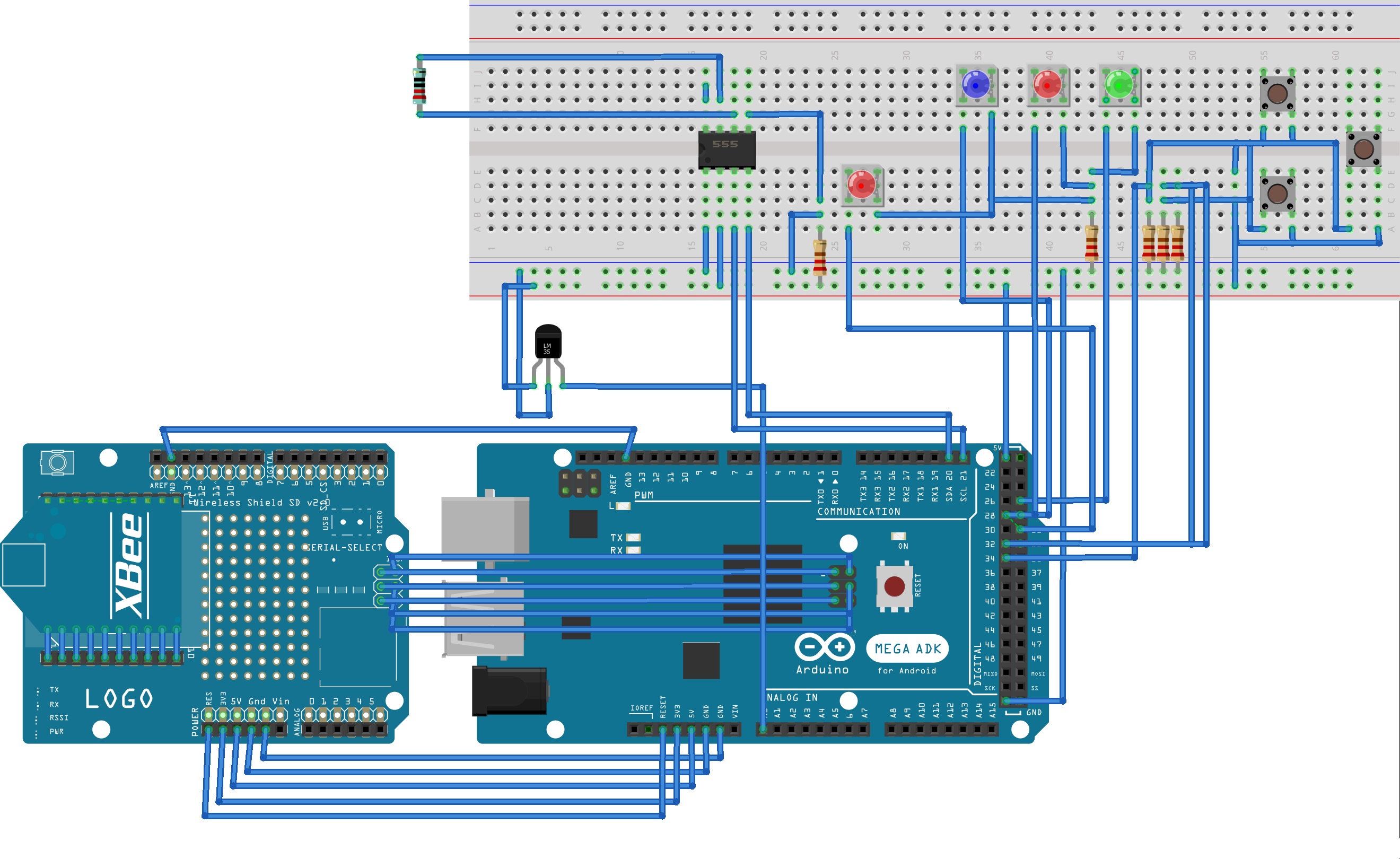
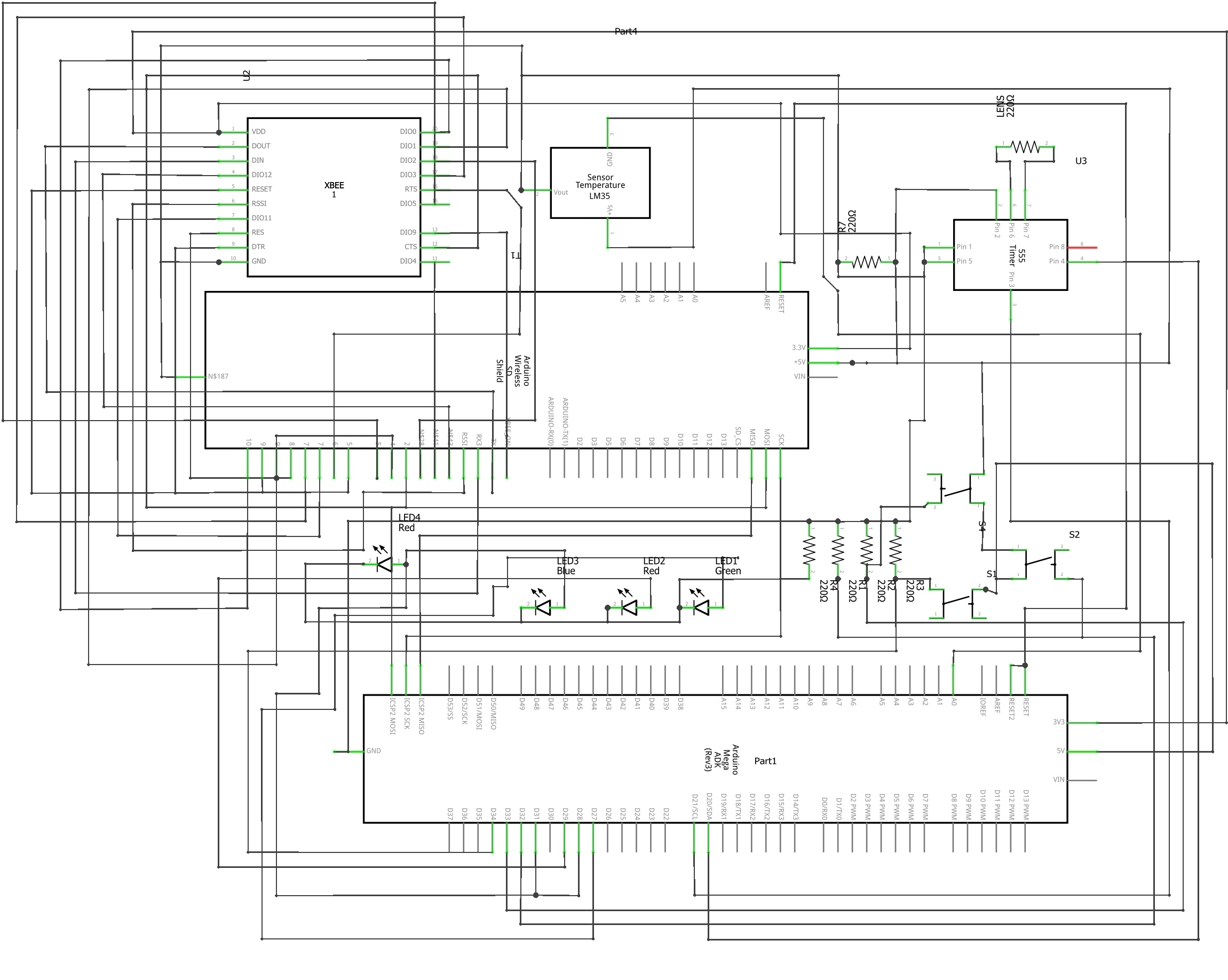
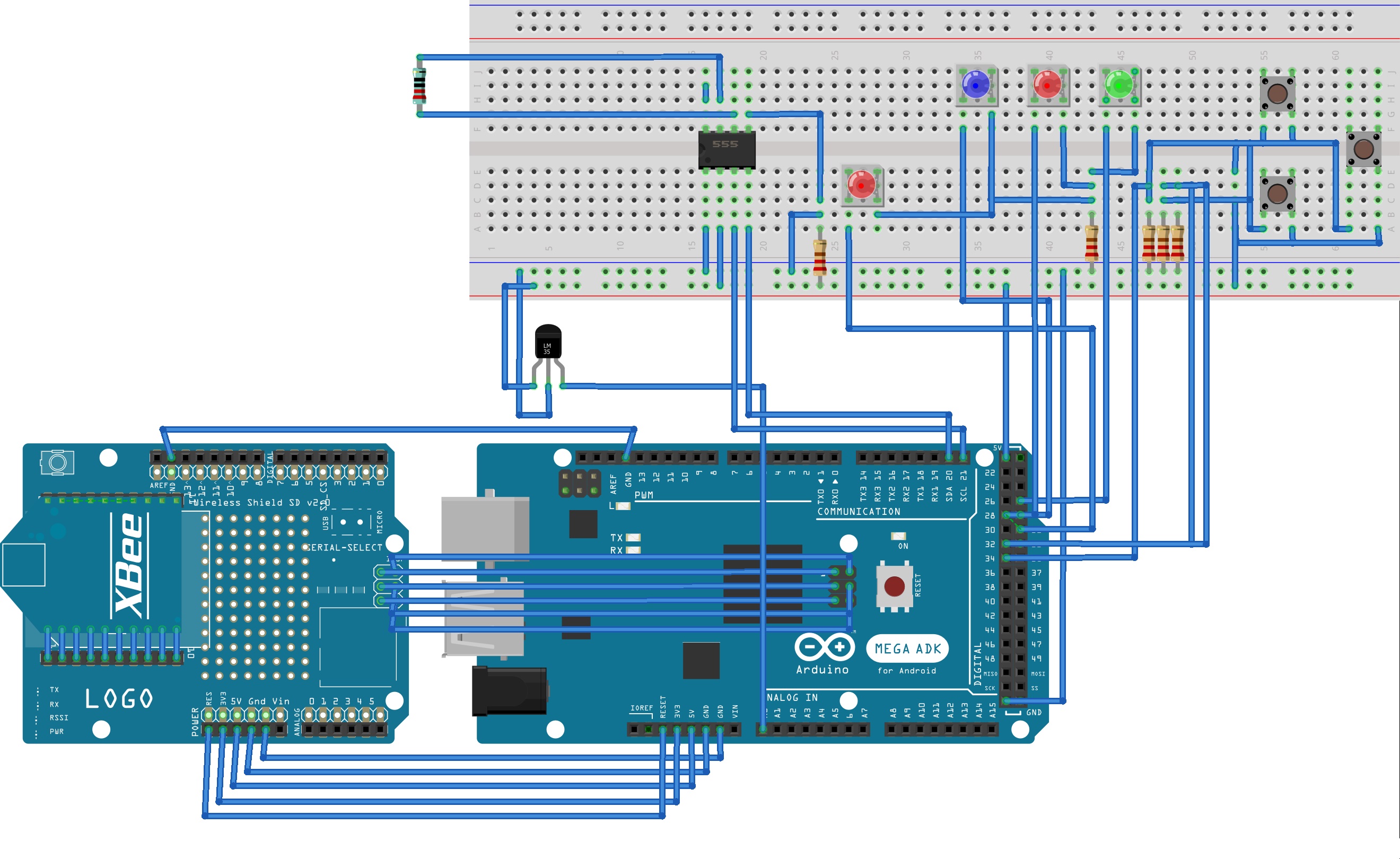
METHODOLOGYThis device will allow people with poor vision to obtain prescriptions with a portable and inexpensive phoropter without the need for an optometrist or an expensive phoropter. Individuals will also be able to dynamically change how they use and interact with these glasses as this device will change the focal length of its lens replacing the need for cumbersome progressive and multifocal lenses. These auto focal glasses would be a better alternative to progressive and multifocal lenses as they wouldn’t restrict the user’s field of vision to see objects in focus. To build these auto focal glasses, a virtual reality headset was used as a frame and a liquid lens was fixed in one of the sockets replacing the preinstalled glass lenses. The LEDs, Tactile buttons, IR receiver, the Arduino Mega 2560, and the HV892 driver was fitted into a small casing made of glass. This enclosure has two wires which connect to the lens in the headset. The device was wired as shown in Figure 1.5 (Schematic view) and Figure 1.6 (Breadboard view). Finished device pictures are shown in Appendix A, Figures 2.1 and 2.2.
The Arduino was programmed to declare variables in the setup and then execute all commands after. Code executed by the device is provided in Appendix E. When executing, the code will initially wait for input and switch to automatic phoropter or auto focal glasses mode based on the input. The code will then ensure that the Arduino turns on an indicator light to show which mode the program is running and executing. When the code is executing the phoropter mode, the lens will be provided roughly 9.8 volts and will change focus correspondingly. The user will then press “up” and “down” buttons on either the IR remote or the tactile buttons on the device itself to increase and decrease the voltage instantly. When signals are received, the code will determine if the user wants to increase or decrease the voltage and will send and calculate the necessary voltage that should be outputted to the lens. After the voltage that should be output is determined, the Arduino sends I2C commands to the HV892 chip to produce the necessary AC voltage for the lens. Once the user feels that optimal viewing experience has been achieved they will press the enter button. The code will then archive the voltage provided into the lens at that time and calculate the user's eye power using the formula: (Official Prescription Power in Diopters) = 0.3235 * (Final Lens Voltage) - 17.8150 (Roy, 2019). When the code is executing the auto focal glasses mode, the program will use an array of the user’s different prescriptions and user input to determine the voltage output to the lens to correct vision for a specific prescription. After voltage output has been determined, the corresponding I2C commands will be sent to the HV892 driver which will change the focus of the lens. At any point, the user can press the up or down button to cycle through the prescriptions in the array. This allows the user to switch which prescription the lens is correcting for depending on what the user is looking at. This device was tested using Snellen’s eye chart and the aid of 50 participants. Snellen’s eye chart is typically used by optometrists to determine a patient’s prescription. The user did not experience any harm when testing the device as no voltage was applied to the body. Data was collected on the participant’s visual acuity without the usage of visual aids. Then the participant’s visual acuity was measured again with the usage of the auto focal glass and the usage of their current visual aid. Analysis of the data was used to determine the percentage improvement in eyesight across all participants. T-tests were used to determine if the auto focal glasses are significantly better than conventional aids for vision such as glasses and contact lenses.
RESULTS & DATA ANALYSISThe purpose of the auto focal visual aid which uses variable focus liquid lenses is to allow the user of the glasses to instantly change the focal length of a variable focus lens to allow for clarity of vision when looking at different ranges, replacing progressive and multifocal glasses. In the experiment which measured visual acuity using Snellen’s eye chart, data was taken on the visual acuity of the participant without the use of any visual aids, with the use of the participants’ current visual aid and with the use of the variable focus glasses. The averages of participants' visual acuity in each scenario are shown in Figure 3.1. The values shown by that bar graph in Figure 3.1 denote how much visual acuity that individuals can see in comparison to 20/20 vision. For example, if the bar height went up to 25, then that individual has 20/25 vision, whereas if the bar height went up to 30 then the individual has 20/30 vision. The raw data taken on the visual acuity of patients is provided in Table 1.1 in Appendix B. A bar graph of each individuals’ visual acuities is shown in Figure 4.1in Appendix C.
ADD AN IMAGEDelete this image When the auto focal glass was used as a visual aid, participants consistently had a visual acuity of either 20/20 or 20/15 showing that the device was able to correct the user’s vision to a high degree of visual acuity without falling short of the 20/20 margin. The visual acuity that a user had with a current visual aid varied more than the visual acuity with the auto focal glasses. This was likely because prescriptions change over time and because users’ current visual aids can not perfectly correct an individual's changing prescription. This may be one reason why the standard deviation of the percentage improvement in visual acuity with the use of current visual aids is higher. There was also an inconsistency in the user’s ability to operate the device which led to differences in the performance of the auto focal glasses across various users. For example, some users who started with worse initial eyesight achieved better eyesight with auto focal glasses than others using the same device. One example of this can be seen in Figure 4.1 in Appendix C between participants 6 and 11. Participant 6 has a better regular vision than participant 11. Participant 6 started with a visual acuity of 20/30 and whereas participant 11 had a visual acuity of 20/100. After using the auto focal glasses participant 6, who started with a higher degree of visual acuity, had visual acuity of 20/20 whereas participant 11 ended up with a higher visual acuity of 20/15. The use of auto focal glasses requires the user to adjust the focal length of the glass. The variability induced by this leads to the differing performances of this device’s ability to correct a user’s vision. Using the data on participants’ visual acuities using conventional visual aids and the auto focal glasses, percentage improvement in visual acuities were found in reference to participants’ original visual acuity (without the use of any visual aids). This was calculated by using the formula: (Visual Acuity Improvement in Feet) / (Original Visual Acuity without the use of Visual Aids in Feet) * 100. Graphs of the average improvement in visual acuity with the use of participants’ current/conventional visual aids versus the use of the auto focal visual aids are shown in Figure 3.2. The average percentage improvement in visual acuity using auto focal glasses (58.06%) is higher than the user of current/conventional visual aids (41.33%).
All the data for each individuals’ percentage improvement in visual acuity is shown in Figure 4.2 in Appendix D. As shown in Figure 4.2 in Appendix D, the auto focal glasses consistently outperformed participants’ current visual aid in terms of improvement in vision except with two participants. With participants 12 and 19, the percentage improvement in visual acuity with the use of auto focal glasses and the use of conventional visual aids were the same. Overall, the auto focal glasses were able to provide a higher degree of visual acuity. This means that auto focal glasses correct a user's vision better than conventional visual aids a majority of the time. The data in Figure 3.2 clearly shows through averages that the percent increase in visual acuity of a participant using auto focal glasses was higher than the percent increase in visual acuity of a participant using their current visual aid. To determine the significance of this difference a 0.05 one-tailed t-test was run. After running the t-test and obtaining a p-value of 0.0041 which was less than the alpha level of 0.05, the null hypothesis was able to be rejected which suggested the alternate hypothesis. This one-tailed t-test shows, with 95% confidence, that there is a significant difference in percent increase in visual acuity when using auto focal glasses as opposed to current visual aids. This means that the auto focal glasses did improve participants’ visual acuity significantly when compared to conventional visual aids. The data associated with performing the t-test are shown in Table 2.1.
As the data in Figure 3.1 shows, the use of current visual aids brings visual acuity of patients to 20/30 or 20/20. The participants’ current visual aids could not increase the degree of visual acuity past 20/20 unless the initial visual acuity is previously higher than 20/20. The only way to achieve a higher degree of visual acuity than 20/20 without using commonly available visual corrections is to go through LASIK eye surgery. One reason the auto focal glasses were able to increase the user’s visual acuity to 20/20 was likely due to the ability to adjust the focal length of the lens and adjust the distance between the lens and the user’s eye. This allows the user to control the path of light to ensure visual clarity. The reason the auto focal glass was able to outperform conventional glasses and contact lenses and achieve better than 20/20 vision was likely due to the smaller aperture of the lens. Due to this smaller aperture of the lens the blur circle, a collection of stray light that reduces visual acuity that typically falls on the back of the retina is reduced. The blur circle is reduced due to the smaller aperture as more stray light is blocked and is the same reason why high degrees of visual acuity can be achieved by looking through a pinhole. Because the diameter of the lens is small this reduction in the bur circle may play a role in allowing the auto focal glass to achieve a visual acuity higher than 20/20.CONCLUSION The goal of this project was to create a device that can effectively integrate a voltage-controlled variable focus lens and microcontroller to automatically change lens curvature with the use of a program. This device would replace phoropters and be used as an autofocus eyeglass that adjusts the focal length of a variable focus lens to allow for clarity of vision when looking at different ranges, replacing progressive and multifocal glasses. After an auto focal glass was created it was used and tested by 50 participants. It was hypothesized that the auto focal visual aid created would improve a user’s vision significantly more than the user’s current visual aids. A p-value of 0.004 was calculated after running a t-test which was less than the alpha level of 0.05. This allowed the null hypothesis to be rejected, suggesting the alternate hypothesis: auto focal glasses significantly improved a user’s vision compared to conventional visual aids. The auto focal glasses likely outperformed other traditional visual aids as the lens has a smaller aperture which allows it to act as a pinhole. This smaller aperture allows stray light to be blocked which improves visual acuity. Another reason why the auto focal glasses outperformed users’ current visual aids was likely because the distance between the lens and the eye can be changed. This improves vision as it allows for finer adjustments made by the user to focus light on to the optic nerve. The performance of the auto focal glasses was inconsistent as the glasses performed differently for users, even if they had the same original visual acuity. This is likely due to the variability in the use of the glasses in terms of the user sending the correct amount of voltage to the lens and positioning the lens the right distance from their eye. Because there are multiple ways to adjust auto focal glasses it may be hard for some users to achieve the most optimal visual acuity with the auto focal glasses. Other research by Ronak Roy establishes a relationship between power in diopters and voltage provided to lens: (Official Prescription Power in Diopters) = 0.3235 * (Final Lens Voltage) - 17.8150. This equation/relationship is important as it can allow for the instant calculation of necessary voltage output to match a user’s prescription. This research is significant as it can allow auto focal glasses to more accurately determine a user’s prescription. Another study performed by Ratnakirti Roy compares the use of different autofocus technologies in digital cameras. This research is significant as it identifies the benefits and consequences of each type of autofocus algorithm. This research is important as it could likely identify more efficient autofocus methods for use in a visual aid. Future research projects that could be pursued with variable focus liquid lenses are making a visual aid that can automatically switch lens focus after determining what the user is looking at. This would allow for a dynamically changing viewing experience that would instantly adapt to the most optimal viewing experience rather than having the user manually change the power of the lens. Other future research that could be done on variable focus liquid lenses is using machine learning to determine a function to relate the AMP value sent to the driver to the actual power of the lens. This study which would be similar to Ronak Roy’s study would allow for accurate measurements of user prescriptions.





{kind=link}
{kind=link}
Comments