


Hardware components | ||||||
 |
| × | 1 | |||
 |
| × | 1 | |||
 |
| × | 1 | |||
 |
| × | 2 | |||
| × | 1 | ||||
Software apps and online services | ||||||
 |
| |||||
Hand tools and fabrication machines | ||||||
 |
| |||||
 |
| |||||
During the Corona (COVID-19) pandemic it became obvious that a lack of medical equipment can cause a severe impact.Often, also simple equipment and designs can be helpful when no professional equipment is available.
This project contains information about an open-source ventilator device. Main purpose of this project is to generate ventilator design files and documentation for situations, when no professional and medical equipment can be obtained. Easy to assemble and available components are used with a clear focus on simplicity, availability and scalability, so local and short notice production is enabled wherever needed around the globe.
The material and documentation here is provided as open source with no warranties explicit or implied. No material on this site is intended to provide medical advice. All designs are intended for investigational use only. This site does not represent any official policies or procedures. The project is provided "as is", without warranty of any kind, express or implied, including but not limited to the warranties of merchantability, fitness for a particular purpose and noninfringement. In no event shall the authors or copyright holders be liable for any claim, damages or other liability, whether in an action of contract, tort or otherwise, arising from, out of or in connection with the software or the use or other dealings in the software. Only use this designs, documentation or any provided information if you accept the above disclaimer.
How does it work?An AMBU-bag is used as pressure reservoir. It already features an O2 inlet (O2 concentration is crucial for patients with acute respiratory syndrome) and several safety features including e.g. overpressure and bypass valves. Being standard for emergency help, these bags are available at substantial volumes. A motorized and microcontroller+sensor controlled setup squeezes the bag at the right pattern, supporting assist-, pressure-, volume- and flow-control ventilation and exhaled gas measurements and filters. Additionally provided design-files for 3D-printed adapters and valves also shall help to fill in gaps 'accessory' supply with professional equipment (secure, that all available equipment can always be used) and/or allow to reduce infection risk of medical personal (e.g. filters and UV lighting to exhaled air) and/or enable best use of professional equipment for critical cases (e.g. switch patient on recovery track to lower requirements open source ventilator). All is based on open source and commonly accessible parts; especially for the mechanics the objective is to be scaleable in production and hence fully 3D-printable. Only the motor and it's screws as well the belt is not printed. BLDC motors are proposed. Also standard stepper motors as NEMA23 are a design in option. Design findings and results are openly shared as part of the open source, so other teams can easily also build upon it.
The Human LungA human lung is a complex organ responsible for gas exchange between the body and the environment. The lung is mainly composed of two types of airways (conductive and respiratory airways), alveoli, and blood vessels.
- Conductive airways: The main role of the conductive airways is to transport the bulk of air from and into the lung. No gas exchange (perfusion) takes place in the conductive airways. This is why conductive airways are also called dead space.Why is this information important? because mechanically, conductive airways are responsible for the resistance to the flow. Thus protecting the lung from high flowrates while inflation and from collapsing during deflation.
- Respiratory airways: These airways differ from the conductive airways by containing alveoli on their walls. Perfusion starts taking place at the respiratory airways. The air at this level is transported via diffusion rather than conduction.Why is this important? during respiration, the air needs to sit long enough in the lung for oxygen to diffuse from the tips of the conductive airways into respiratory airways. Same for carbon dioxide to diffuse from the respiratory airways into the conductive airways. This set the criteria for picking the ventilation periods for inhaling and exhaling.
- Alveoli: At the tip and the walls of the respiratory airways, alveoli are located. The group of alveoli form an acinus, which in return form the sponge like consistency of the lung. Each alveoli is surrounded by blood vessels. The common wall between the alveolus and the blood capillaries offers the medium for oxygen and carbon dioxide be exchanged.Why is this important? Diseases such Covid-19 lead SARS (Severe Acute Respiratory Syndrome) or ARDS (Acute Respiratory Distress Syndrome) via the inflammation in the lung. Which means water starts building up in the alveoli. Thus reducing or preventing the perfusion of the lung. This is a critical stage, where patients will need to be put on assistant/mechanical ventilation. Physicians will use different methods to keep the alveoli open, recruit the collapsed ones and bring the inflation down, all while not damaging further the alveolar wall.
Mechanical ventilator is a medical device used to assist or replace spontaneous breathing.
Mechanical Ventilator Functionalities
In the following section we list the main functionalities of a mechanical ventilator. We also aim to translate these functionalities into design requirement. As we aim in this work to address crucial need for supporting the high demand for mechanical ventilators during crisis times. The following functionalities aim to support the physicians with the right tools to treat patients suffering form SARS & ARDS:
Tidal Volume: Is the volume of ventilated air at each respiratory cycle. An average adult at rest would need any where between 500 to 800ml of tidal volume each respiratory cycle to properly ventilate the lung.From requirements point of view, this means the ventilator need to:
- pump up to 800ml of air
- control the pumped volume
- monitor and report if the pumped volume exceeded to dropped below the critical tidal volume
Pressure: The pressure produced by the lung ventilators is responsible for driving the air into the lung and controlling the rate of exhaling of the lung.From requirements point of view, this means ventilators need to:
- control the pumping pressure
- monitor and report if the pressure exceeds critical levels, to protect the lung from VALI (Ventilator-Associated Lung Injury)
- control the PEEP (Peak End Expiratory Pressure), which protects alveoli from collapsing
Fraction of inspired Oxygen (FIO2): To protect the lung from VALI, the physicians could choose to ventilate the lung with lower tidal volume but higher oxygen content. For that the ventilator is connected to an oxygen intake.From requirements point of view:
- The ventilator needs to control the mixture fracture of oxygen and air, which will be ventilated into the lung
- Monitor the concentration of oxygen in the pumped gas. This value is used to adjust the FIO2 and to compare it with the oxygen level in the blood. Which in return is an important indicator of oxygen transfusion.
Expired Carbon-Dioxide: Carbon dioxide is toxic for humans. The concentration of the expired CO2 is an indicator if the patients lung is being well perfused and ventilated. Physicians track CO2, for example, to know if the patient is still alive.From the requirements point of view this means:
- Monitor and report the CO2 concentration of exhaled air.
In interviews with medical personal we noticed that in most cases of of intensive care the pressure contol is the mode chosen. Thats why we will focus on this method in the following prototype.
A control loop will keep the pressure level at a preset value. A certain volume (l/min) will arise. In case needed the medical personal will adjust the pressure level to increase or lower the volume/min. Also the ratio of pressure to volume/min is a indication of the human lungs health.
MechanicsAll mechanical parts are either standard parts (such as screws) or 3D printrd parts.The files can be found here.The belt is build out of tape which is simply folded and therefore no sticky to external surfaces anymore.
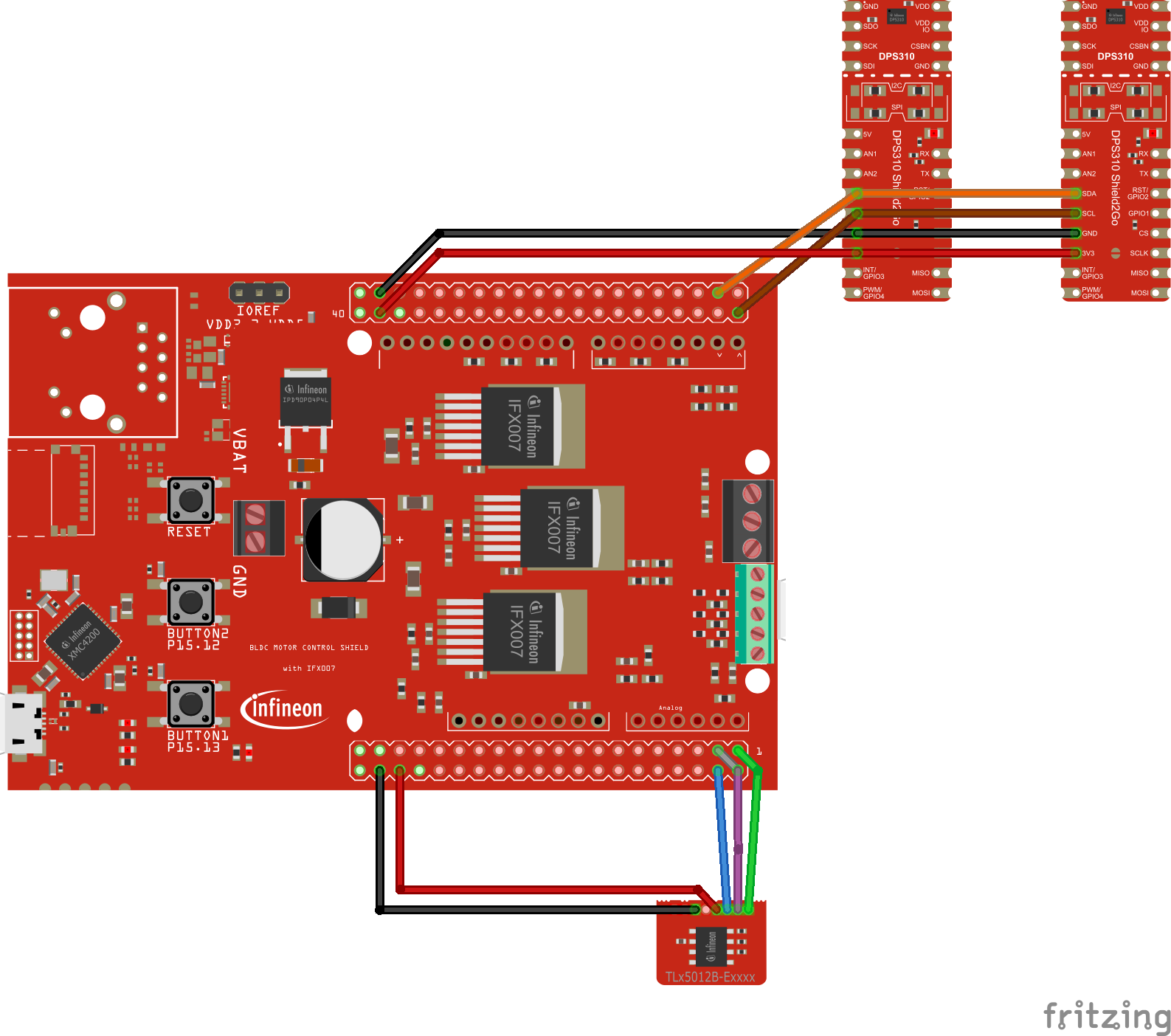
ElectronicsThe electronic setup involves
- microcontroller (XMC4700 relax kit) in charge of sensor readings, motor control and pressure control loop
- Power stage driving the motor (IFX007 BLDC shield for Arduino)
- Angle sensor (TLE5012B S2GO breakout board) monitoring the motor rotor position
- Digital pressure sensor monitoring pressure and air flow (DPS368 S2GO boards)
In pressure controlled mode there can be slow speeds even up to 0 with still need to hold the pressure in the lung. To maintain a high torque at lower speeds we decided to build a sensor based closed loop motor control setup. The rotor position is detected by a TLE5012B magnetic angle sensor. This way you can set the half bridges of the IFX007 power stage in the right way to create the needed magnetic field to move or hold the rotor.We use this sensor as well to detect upper and lower endpoints so we don't turn the motor to far.
In our pressure and flowmeter setup we use two DPS368 S2GO boards.The DPS368 (digital pressure sensor) is waterpoof and can monitor pressure levels as accurate as 6Pa. We placed the two sensors along a tube setup.This way we can calculate the flow according to the pressure drop (loss) across the tube. We tested 4mm/6mm/8mm tubes with a length of 80mm between the sensor outlets. The 8mm one showes the best result in terms of sensing accuracy and less pressure drop.In addition we can use one of the pressure values directly for our pressure control loop.
Here you can see the two control loops running. - the closed loop motor control using hte magnetic angle sensor- the closed loop pressure control using the digital pressure sensor
In this clip we showcase the pressure control loop seeting different pressure values. You can see how the pressure (blue) adjusts accordingly. Also in red you can see the flow during inhalation and exhalation phase.










{kind=link}
Comments
Please log in or sign up to comment.